
Introduction
- Click on menu point "1" (in the menu above or below) when you're all set!
- Pay attention to these sticky notes. They'll help you here and there throughout the case.
Wait a sec. Is your toolbox filled? If not, then...
Download the Algorithm Download the Canvas
You may also want to watch this short introduction video.
This case study is about Maya, a 41-year-old lady diagnosed with Multiple Sclerosis two years ago. Maya currently has problems with walking. The content is set at medium level, so the case is a nice way to continue developing your clinical reasoning skills.
Disclaimer
This case study is based on a real patient case. However, the content is simplified to maintain focus on learning the basics of the HOAC II way of clinical reasoning. If you feel like brushing up your knowledge about MS before you start, browsing through PubMed Health or some of our references may come handy.
Initial data (referral & medical record)
Actions to take
Activate your knowledge base
- You already received information on the patient's pathology, age and gender in the introduction. Take a few moments to hypothesise in your mind on the types of problems you expect the patient to have and what factors may cause them. You could base your ideas on knowledge or previous experience.
- Once you are ready, continue to the next step of the actions to take: 'Review the patient demographics'.
Review patient demographics
- Review the case details below.
- Record the case details in your paper version of the Canvas as advised in the Italics below.
- It's a good idea to check the yellow sticky notes next to the case details - they'll help you throughout the case.
Canvas - 'Initial Data' sheet: fill in the boxes on the top part of the sheet.
Canvas examplePrepare data collection
- Prepare for a hypothesis-driven data collection. It is a good idea to use the ICF Core Sets as the basis. Download the applicable Core Sets here.
- Begin to hypothesise on what activity limitations & participation restrictions the patient most likely has.
- Begin to hypothesise on probable underlying impairments and contextual factors.
- Record the guidelines and other evidence you plan to use in the case.
ICF Core Set - select the domains most relevant for the case.
Canvas - 'Initial Data' sheet - 'Guidelines, evidence & remarks' box: make relevant notes.
Reflect, review & continue
- Read the 'Solution' and click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 2.
- A brief and a comprehensive Core Set are available for MS - we'll use the brief Core Set in this case.
- Knowing about the medication may give vital clues about the patient. Read more about Natalizumab here; Venlafaxine is an anti-depressant.
Case details
Maya is a 41-year-old woman diagnosed with multiple sclerosis (MS) two years ago. The neurologist redefined the diagnosis from relapsing-remitting MS to secondary progressive MS three months ago. Over the last months Maya has become very concerned about her decreased walking capacity, which increasingly limits her participation in everyday family life. She has been referred for a 17-day multidisciplinary inpatient rehabilitation.
Basic information & medical history
Height 160cm, weight 53kg. Maya first noted right-sided lower extremity weakness and upper extremity clumsiness two years prior to the MS diagnosis. Maya's current medication include Natalizumab infusions in four week intervals. She also takes Venlafaxine. No other significant past medical history.
Personal & environmental factors
Maya lives with her husband, three children (aged 2, 4 and 11) and a dog in a single story house. Until one year ago, Maya worked in a small grocery shop until and currently receives pensioners' care allowance.
Rehabilitation programme
Individual appointments are scheduled with a neurologist, physical therapist and occupational therapist. Within the multidisciplinary team the PT is the main contact person for Maya.
Solution, rationale & evidence
Solution
The relevant categories in the brief ICF Core Set for MS (accessed 15 November, 2011) for an ambulation problem in Maya's case include:
- b130 Energy and drive functions
- b152 Emotional functions
- b280 Sensation of pain
- b730 Muscle power functions
- b735 Muscle tone functions
- b760 Control of voluntary movement functions
- b770 Gait pattern functions
- d230 Carrying out daily routine
- d450 Walking
- d455 Moving around
- d640 Doing housework
- d760 Family relationships
Rationale & evidence
The selection of the ICF categories is based on the neuromuscular, musculoskeletal, somatosensory and cognitive & perceptual impairments that contribute to gait parameters (Shumway-Cook et al. 2012, see chapters 14 & 15).
Interview & Problem list
Actions to take
Review collected data
- Review the data collected in the interview and informal observation from the Case details below.
- Record the collected data.
Canvas - 'Initial Data' sheet -'Interview & informal observation' box: Note the data in your preferred way.
Canvas exampleGenerate existing problem list
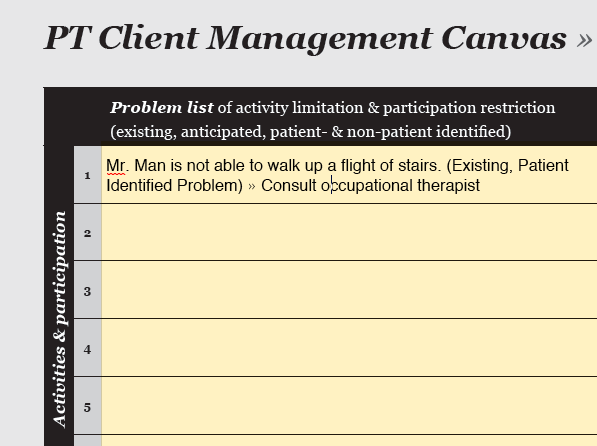
- Describe the existing Patient-Identified Problems (PIPs) in patient-orientated terms.
- In some cases you may already identify existing non-PIPs (NPIPs).
- Notice that in cases where the patient is unable to communicate, the problem list consists only of NPIPs.
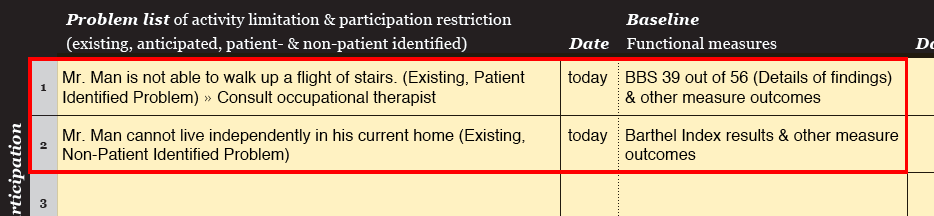
Canvas - 'Problem Tracking' sheet - 'Problem list': Note all problems.
Generate anticipated problem list
- Describe any anticipated Patient-Identified Problems (PIPs) in patient-orientated terms.
- In some cases you may already identify anticipated non-PIPs (NPIPs).
- Notice that in cases where the patient is unable to communicate, the problem list consists only of NPIPs.
Canvas - 'Problem Tracking' sheet - 'Problem list': Note all problems.
Hypothesise on underlying factors
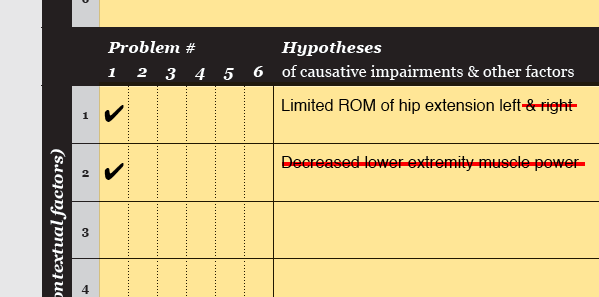
- Hypothesise on the impairments (and Contextual factors) underlying each problem.
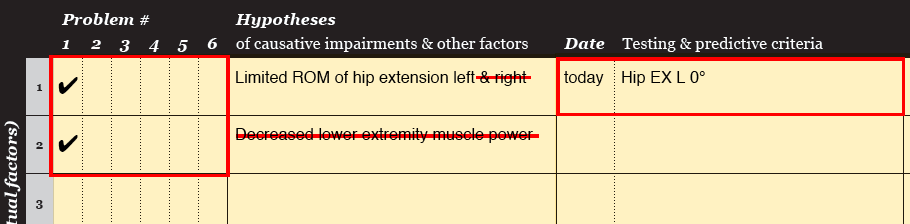
Canvas - 'Problem tracking' sheet - 'Hypotheses' column: list the causative factors and tick the Problem # they are related to.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 3.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Keep it up! You're just starting to get your clinical reasoning skills up to speed !:-)
- Hypothesising on the underlying factors is super important. Those ideas form the basis of the whole case. So get your brain cells fired and working!
Case details
Maya's walking capacity has decreased notably in the last six months. She no longer goes shopping, walks the dog or goes on day trips with her family - she spends most of her time at home. Maya says she can maximally walk just over 10 meters without stopping and that walking is very slow. She prefers to use one crutch on her left when walking outdoors to have the right arm free. She does not need the crutch indoors but often uses the walls for support. Maya manages two steps from the kitchen to the living room by holding onto the wall. When she is fatigued, she goes on all fours.
Maya has to concentrate a lot on each step she takes. She especially has difficulties with her right leg and feels that she is dragging the leg with her. Maya falls every week, most times by stumbling over rugs because she cannot lift her right leg or because her legs suddenly 'give in'. Luckily the falls haven't led to injuries.
Maya complains of low back pain on the right when walking, it is relieved when lying down. The pain has increased within the last month. When Maya walks longer distances and when she is fatigued, her right leg often begins to tremble. During the last couple of months, Maya has noticed that her legs are stiff in the mornings.
Maya feels increasingly fatigued and fatigue limits her everyday life, some days more and some days less - the pattern is unpredictable.
Personal & environmental factors
Maya lives her life with MS day-by-day. Up to her late 20s Maya was a skier competing at national level. She finds it difficult to accept that she cannot do sports anymore. Maya says her children are her hobby. Maya's husband works full-time but her mother helps Maya with housework when possible.
Maya does not have individual physical therapy but takes part in an exercise group for persons with MS once a week. Maya has an adjusted car where she does not need to use the leg pedals. Apart from the two crutches, she doesn't have other assistive devices. She does not seem to think she would need extra assistive devices for the duration of the rehabilitation period.
Expectations & concerns
"I would like to be able to walk 60m without stopping on flat concrete surface using one crutch. That's the distance to my favourite place in our yard to sit and watch my children play. If I can walk that distance I could also think about driving to the small local shop and go do a bit of grocery shopping. My husband says that he is afraid that my physical condition will deteriorate even further and I can’t take care of housework and my children.”
Informal observation
Maya has walked approximately 15m to the treatment room without showing signs of fatigue. Maya relies heavily on the crutch for support and the gait is asymmetrical. She limps with a stiff knee. Her upper body is completely tensed and when asked to look to the sides, she completely stops walking before she turns her head to look around. Maya gets a little emotional when she talks about her children and family life. No apparent cognitive deficits.
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; NPIP = non-patient identified problem; OT = occupational therapist; ROM = range of motion
Fatigue was not included in the hypotheses because of its complex nature and difficulty to measure different components of fatigue (Bradley et al. 2010). In addition, in a recent Cochrane review exercise therapy was not been found to alleviate fatigue (Rietberg et al. 2011).
Rationale & evidence
The justifications for inclusion of anticipated problems in the problem list were discussed with Maya before placing it in the problem list. They included:
- P4: As Maya estimates her maximal non-stop walk distance to be just over 10m, it is reasonable to believe that she is not able to move around the large rehabilitation centre without a wheelchair without getting excessively fatigued.
- P5: Based on the interview, Maya's husband has raised concerns that Maya’s deteriorated physical capacity and increased fatigue have decreased her social functioning and quality of life (QoL). Persons with MS (pwMS) whose disease is more severe, who receive disability pension or who have children to care for are typically less physically active (Beckermann et al. 2010). As gait, disability, hypertonia of lower limbs and fatigue negatively affect quality of life, treatment with an emphasis on physical conditioning, gait and fatigue should be considered to improve QoL in pwMS (Nogueira et al. 2009).
- P6: Based on the interview, it is apparent that Maya does not receive the health care and social support she requires for maintaining her physical capacity and QoL. For example, as Maya's lower extremities are stiff in the mornings, it is reasonable to believe that her muscle tone is increasing. Because pharmacological treatment is the main treatment for spasticity (Smania et al. 2010), it is important to ensure that Maya knows when to approach her neurologist. Maya does not have adequate assistive devices, she does not receive individual physical therapy sessions or help with housework.
- The hypothesised underlying factors are based on neuromuscular, musculoskeletal, somatosensory and cognitive & perceptual impairments that contribute to gait parameters (Shumway-Cook et al. 2012, ch. 14 & 15).
Examination strategy
Actions to take
Formulate examination strategy
- Review the Case details below.
- Formulate an examination strategy to assess the extend of the identified problems. Use tests and measurements at activity & participation level.
- Formulate an examination strategy to assess if the hypothesised underlying factors are correct. Use tests & measures mostly at body functions & structures level.
Canvas - 'Examination' sheet - 'Tests & measurements': note the tests & measurements.
Canvas exampleSeek consultation if needed
- When it is not possible to generate an examination strategy for a problem or an underlying factor, seek consultation from other health care professionals.
Canvas - 'Problem tracking' sheet - 'Problem list' / 'Hypotheses' columns: Note the need for consultation next to the relevant problem / causative factor.
Canvas exampleReflect, review & continue
- Click 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 4.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Are you already giving all those brain cells a good work out? "No ideas of causation, no examination strategy..."
Case details
The following problems (P) were identified:
- P1: Maya is not able to walk with 1 crutch 60m non-stop on flat hard surface outdoors. (PIP-E)
- P2: Maya walks slowly. (PIP-E)
- P3: When walking more than 10m, Maya has low back pain on the right. (PIP-E)
- P4: Maya is not able to transfer from place to place in the rehab centre by walking. (NPIP-E)
- P5: Deteriorated physical capacity decreases Maya's quality of life. (NPIP-A)
- P6: Maya does not receive the physical therapy, occupational therapy or social services she requires. (NPIP-A)
The following underlying factors were hypothesised (H):
- H1 Disturbed gait pattern functions are related to P1 - P5
- H2 Decreased postural control is related to P1 - P5
- H3 Decreased LE muscle force production capacity is related to P1, P2, P4, P5
- H4 Disturbed proprioception is related to P1, P2, P4, P5
- H5 Increased LE muscle tone is related to P1, P2, P4, P5
- H6 Limited LE ROM is related to P1, P2, P4, P5
- H7 Low self-efficacy is related to P1, P5
- H8 Insufficient assistive devices is related to P4
- H9 Insufficient support from health authorities is related to P6
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; NPIP = non-patient identified problem; OT = occupational therapist; ROM = range of motion; PSCQ = patient-specific complain questionnaire; VAS = Visual Analogue Scale; MSWS-12 = Multiple Sclerosis Walking Scale - 12; 25FWT = 25-foot (7.62m) Walk Test; w/ = with; SF-36 PCS (physical component summary score); SF-36 MCS (mental component summary score); OGA = Observational Gait Analysis; BBS = Berg Balance Scale; MRC-scale = Medical Research Council Scale; MAS = Modified Ashworth Scale.
Rationale & evidence
The relationship between gait parameters and impairments is complex and depends on the extend of the impairments, functional level and compensation capacity of the other systems (Shumway-Cook et al. 2012). The following measurement instruments were chosen to reflect a range of activity & participation and body functions & structure measures:
Activities & participation
- Patient-Specific Complaint Questionnaire (PSCQ) is used to identify and evaluate the extend of functional limitations (Keus et al. 2004). In Maya's case the PSCQ consisted of measuring maximal non-stop walking distance (in meters) outside on flat concrete surface. In addition time (in minutes) was recorded and the Visual Analogue Scale (VAS) was used to assess effort and low back pain.
- Multiple Sclerosis Walking Scale (MSWS)-12 measures self-reported walking difficulties in everyday life (Hobart et al. 2003, Motl et al. 2008, Bladh et al. 2011). The MSWS-12 consists of 12 items scored at a scale of 1-5 with a total sum of 60 points indicating the highest limitation and 12 no limitation.
- 25ft Walking Test (25FWT) at maximal speed from a static start with 1 crutch was used for measuring gait velocity in Maya's habitual walking style. The test perfectly resembles relevant daily life situations such as crossing an intersection (Gijbels et al. 2011).
- 25ft Walking Test (25FWT) at maximal speed from static start (Gijbels et al. 2011) with 2 crutches was used to evaluate gait velocity when Maya has more symmetrical support from crutches (Shumway-Cook et al. 2012).
- SF-36 scale was used to measure various aspects of health-related quality of life (QoL). The scale has been widely used in QoL studies carried out in MS patients (Nogueira et al. 2009). The SF-36 is a generic scale consisting of 8 sub-scales that can be used independently (Dallmeijer et al. 2007). 50 points is considered the norm.
Body functions & structures
- Observational Gait Analysis (OGA): for assessment of disturbed gait pattern functions and kinematic patterns of movements (Shumway-Cook et al. 2012).
- Berg Balance Scale (BBS): for assessment of postural control. In Maya's case the BBS is used for assessment of a hypothesis of an underlying problem in gait and therefore treated as a testing criteria.
- Upright motor control test: for assessment of ankle, knee and hip flexion & extension strength in standing position (Shumway-Cook et al. 2012).
- Joint position & joint motion: for assessment of proprioception (Shumway-Cook et al. 2012).
- Modified Ashworth Scale (MAS) and clonus testing: for assessment of muscle tone and clonus.
- Passive ROM: for assessment of passive range of motion.
Consultation
It was not possible to create a comprehensive examination strategy for the following underlying factors:
- Low self-efficacy: referral to psychologist for consultation.
- Insufficient assistive devices: referral to occupational therapy for consultation.
- Insufficient support from health authorities: referral to rehabilitation social services for consultation.
Examination findings
Actions to take
Review & analyse findings
- Review the examination findings from the Case details below.
- Record the examination findings. Aim to include only the most important findings in the Canvas.
- Analyse whether the findings support or refute the identified problems and hypothesised underlying factors.
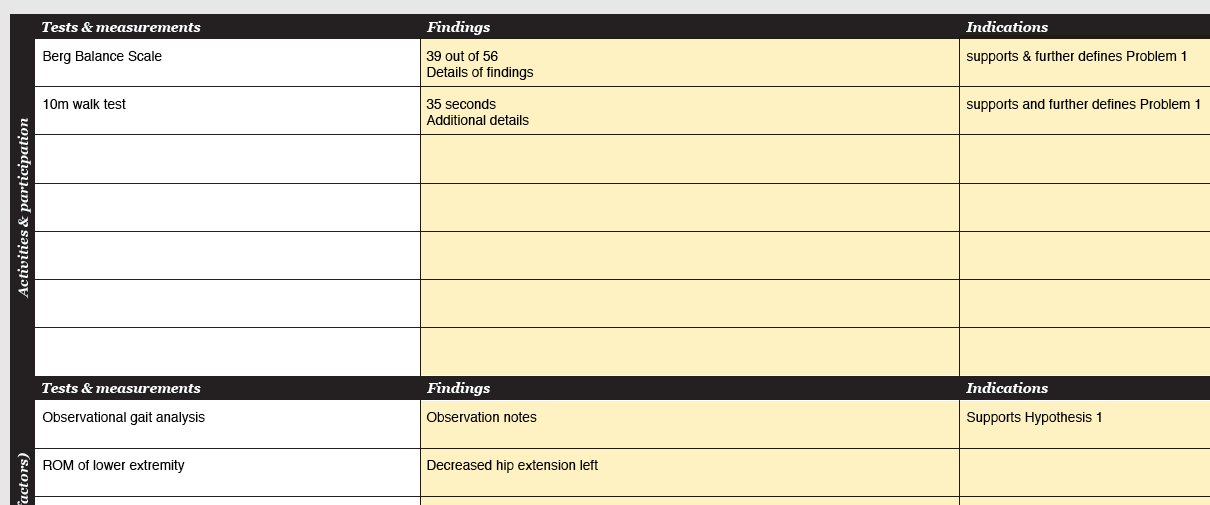
Canvas - 'Examination' sheet - 'Findings' column: record the findings.
Canvas - 'Examination' sheet - 'Indications' column: note whether the findings support or refute any of the identified problems and hypothesised underlying factors.
Refine underlying factors
- Refine the hypothesised underlying factors and cross-out the refuted ones.
- (When the findings do not provide enough information for you to accept or refute the hypothesised underlying factors, carry out additional examination procedures following the same procedure as outlined in the 'Examination strategy'.)
Canvas - 'Problem Tracking' sheet - 'Hypotheses' column: refine /cross-out hypothesised underlying factors.
Add NPIPs
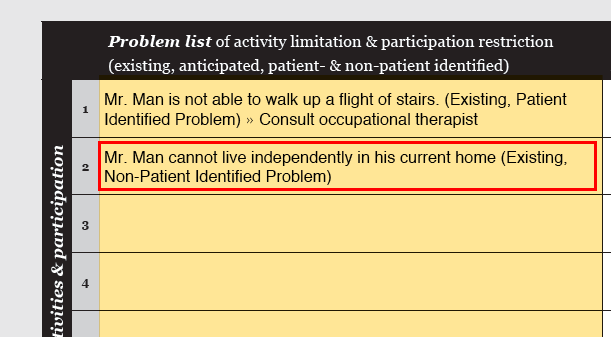
- Often (additional) Non-Patient Identified Problems (NPIPs) are identified in the examination. Now that the examination is completed, all NPIPs should have been identified. Note whether the NPIPs are existing or anticipated.
Canvas - 'Problem tracking' sheet - 'Problem list' column: add NPIPs.
Canvas exampleHypotheses & rationale
- From this point on the accepted underlying factors are called hypotheses. The reasons as to why an anticipated problem is justified is called rationale.
- Check that each existing problem is linked to hypotheses. Note the baseline measure of the underlying impairments.
- Check that you have identified rationale for each anticipated problem.
- If you decide to consult another health care professional, document the reason.
Canvas - 'Problem Tracking' sheet - 'Hypotheses' column: Link all problems to hypotheses or rationale. Elaborate on the rationale e.g. on the backside of the problem tracking sheet.
Canvas - 'Problem Tracking' sheet - 'Baseline' column: Note the baseline of the examination measurements for each hypothesis.
Refine problem list
- Identify problems that should be treated by other health professionals, remove them from the problem list and make a referral.
- Identify problems that cannot be fully resolved and modify the problem statement.
- Any changes in the PIPs should only be made after a discussion with the patient. Notice that after this step PIPs and NPIPs are treated the same way.
- Note the baseline measures for all retained problems.
Canvas - 'Problem Tracking' sheet - 'Problem list': Refine the problems if necessary.
Canvas - 'Problem Tracking' sheet - 'Baseline' column: Note the baseline measures for each problem.
Reflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 5.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- The clinical reasoning steps in this section very much relate to one another and help you work toward the final problem list and hypothesis & rationale list. Precise and specific lists will make the rest of the clinical reasoning process flow by!
Case details
The following data was attained in the examination:
Activities & participation
- PSCQ walking outside with 1 crutch: maximal non-stop distance 42m; time 2:35min; VAS (effort) 80/100mm; VAS (low back pain) 70/100mm
- MSWS - 12: 47/60
- 25FWT at maximal speed from static start with 1 crutch: 11.5 sec
- 25FWT at maximal speed from static start with 2 crutches: 12.3 sec
- SF-36: PCS (physical component summary score) 28.6, MCS (mental component summary score) 38.2
Body functions & structures
- OGA: Right LE stance phase - initial contact on heel; mid-stance knee hyperextension and forward lean of the trunk; single-limb support short, no full weight bearing on R; Trendelenburg leading to L pelvis falling down; limited hip extension; no toe-off. Right LE swing phase - hip circumduction with trunk lean L; toe drag.
- BBS: total score 39/56 - specific items - sit to stand 4; stand to sit 4; transfers 4; standing 2 min 4; sitting 4; standing feet together 1 (needs support to get to position); standing eyes closed 3 (requires supervision); functional reach 3 (22cm); look over shoulder 3 (weight not fully shifted to R); slipper reach 3 (requires supervision); 360 degree turn 2 (R 21.3 sec, L 12.0 sec); stool touch 1 (2 steps with minimal support from PT); tandem stand 3 (can place foot ahead independently and stand 30 sec, R foot in front); one-foot stand 0 (R 0 sec, L 15.0 sec).
- Upright motor control test: knee extension – R weak (unable to support body weight on the flexed knee), L normal; knee flexion – R weak (needs >10 sec to complete 3 repetitions), not possible to test L as cannot stand on one foot on R.
- Isometric force generation – MRC-scale: all R LE muscle groups ≤3/5, m. peroneus 1/5; all L LE muscle groups 4/5.
- Joint position & joint motion: 100% correct. Needs to concentrate a lot to determine joint motion.
- Modified Ashworth Scale (MAS): R + L 0/4. Clonus +/+.
- Passive ROM – lower extremity: full R + L
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; NPIP = non-patient identified problem; OT = occupational therapist; SW = social worker; ROM = range of motion; PSCQ = patient-specific complain questionnaire; VAS = Visual Analogue Scale; MSWS-12 = Multiple Sclerosis Walking Scale - 12; 25FWT = 25-foot (7.62m) Walk Test; w/ = with; SF-36 PCS (physical component summary score); SF-36 MCS (mental component summary score); OGA = Observational Gait Analysis; BBS = Berg Balance Scale; MRC-scale = Medical Research Council Scale; MAS = Modified Ashworth Scale; R = right; L = left; UMCT = Upright Motor Control Test.
Rationale & evidence
Rationale for hypotheses:
- H1 - H3 are accepted based on the findings in OGA, BBS, upright motor control test and manual muscle testing using the MRC-scale.
- H4 and H6 are refuted based on the findings in joint position & joint motion testing and passive ROM.
- H5 is partly refuted based on the findings in MAS and clonus testing.
- (H7 and H8 A psychologist and occupational therapist were consulted already before examination.)
Rationale for refining the problem list
- P4 Based on the findings in the PSCQ, Maya needs a wheelchair to transfer from place to place in the rehabilitation centre. The problem is removed from the problem list and referred to the occupational therapist.
- P6 Based on the interview and complete examination findings, the need for review of the health care services she requires / receives at this point in time and in the future is apparent. Maya was already referred. The problem is removed from the problem list.
Goals
Actions to take
Specify existing problems
- Review the Case details below.
- Establish goals for all problems by setting a target level for the functional measures. Determine when you can expect the patient to meet the goal and set dates of reassessment accordingly.
- Establish testing criteria for each hypothesis. Determine when you can expect the patient to meet the testing criteria and set dates of reassessment accordingly.
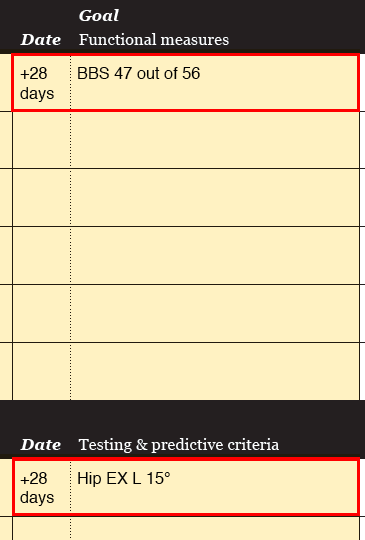
Canvas - 'Problem Tracking' sheet - Goal column: Note goals for functional measures and testing criteria. Note dates of reassessment.
Canvas exampleSpecify anticipated problems
- Establish predictive criteria for each anticipated problem. Determine when the predictive criteria should be achieved for the problem to be eliminated. Set dates of reassessment accordingly.
Canvas - 'Problem Tracking' sheet - Goal column: Note goals for functional measures and predicitive criteria. Note dates of reassessment.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 6.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- When you follow the points in the 'Actions-to-take' list, you will automatically have the basis of your SMART- goals on the Canvas. Smart, isn't it!
- Despite of the smart Canvas, writing SMART-goals can be a little tricky sometimes. You could check this practical guide (Bovend'Eerdt et al. 2009) for extra advice. Step 1 is about writing SMART-goals.
Case details
Maya's goals and concerns
"I would like to be able to walk 60m without stopping on flat concrete surface using one crutch. That's the distance to my favourite place in our yard to sit and watch my children play. If I can walk that distance I could also think about driving to the small local shop and go do a bit of grocery shopping. My husband says that he is afraid that my physical condition will deteriorate even further and I can’t take care of housework and my children.”
The final problem list (E= existing, A = anticipated)
- P1: Maya is not able to walk with 1 crutch 60m non-stop on flat hard surface outdoors. (E)
- P2: Maya walks slowly. (E)
- P3: When walking more than 10m, Maya has low back pain on the right. (E)
- P5: Deteriorated physical capacity decreases Maya's quality of life. (A)
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; NPIP = non-patient identified problem; OT = occupational therapist; ROM = range of motion; PSCQ = patient-specific complain questionnaire; VAS = Visual Analogue Scale; MSWS-12 = Multiple Sclerosis Walking Scale - 12; 25FWT = 25-foot (7.62m) Walk Test; w/ = with; SF-36 PCS (physical component summary score); SF-36 MCS (mental component summary score); OGA = Observational Gait Analysis; BBS = Berg Balance Scale; MRC-scale = Medical Research Council Scale; MAS = Modified Ashworth Scale; R = right; L = left; UMCT = Upright Motor Control Test.
Rationale & evidence
When a goal was set to achieve an improvement, the measure was set to reflect minimal detecable changes. Several reference values for minimal detectable changes specific for persons with MS (pwMS) are available (Paltamaa 2008). When they were not available, the general rule of 20% change was applied (Schwid et al. 2002).
The SF-36 and MSWS-12 are used as a predictive criteria for P5 (Deteriorated physical capacity decreases Maya's quality of life). The reassessment date is set at 3 months with an acknowledgement that reassessment requires that Maya is able to see a PT regularly in her home environment. Regardless, the measure functions as a reference value for future inpatient rehabilitation periods.
Intervention strategy
Actions to take
Plan intervention strategy
- Review the Case details below.
- Plan the intervention strategy. Briefly explain why the strategy should lead to changes in testing & predictive criteria.
- Consider the environmental factors given in the Case details when planning the interventions.
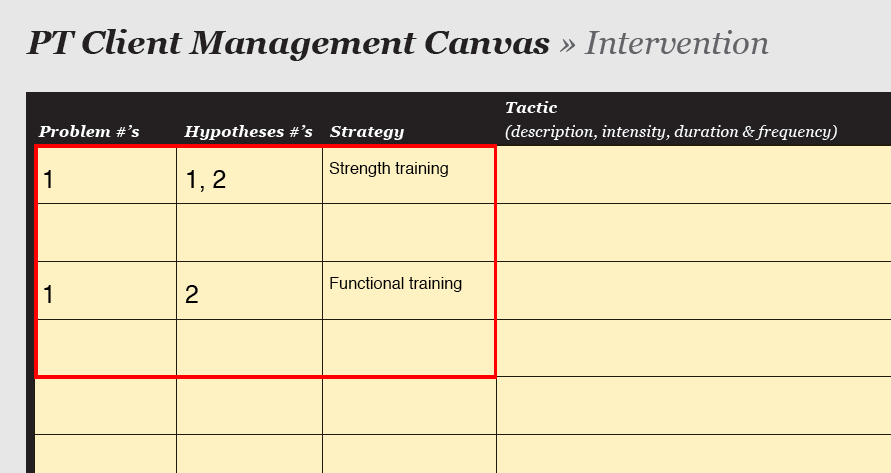
Canvas - 'Intervention' sheet - 'Strategy': Note the strategy and (very) brief reasoning for it.
Canvas examplePlan tactics
- Plan the tactics and relate each tactic to a hypothesis.
- Specify progression.
- Specify the implementer.
Canvas - 'Intervention' sheet - 'Tactics', 'Progression & Remarks', 'Implementer': Note the relevant information.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 7.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- "Success comes from knowing that you did your best to become the best that you are capable of becoming." (John Wooden) :-)
Case details
Goals
- Maya is able to walk 60m (using 1 crutch) non-stop on flat hard surface outdoors with VAS (effort) 80/100mm by the end of the rehabilitation period.
- Walking difficulties cause less inteference in Maya's everyday life. In the MSWS-12 she gets 38/60 points by the end of the rehabilitation period.
- Maya is able to walk 25FWT with 1 crutch in 9.2 sec and with 2 crutches in 9.8 sec by the end of the rehabilitation period.
- When walking the maximal possible distance, Maya has minimal low back pain and when measured with the VAS (low back pain) she scores 30/100mm by the end of the rehabilitation period.
- Maya slightly improves her physical capacity and thereby her quality of life. In the SF-36 she scores PCS 34.3 and MCS 45.8 and in the MSWS-12 she scores 38/60 in 3 months time.
Testing criteria
- Improved gait pattern: OGA right LE weight-bearing; toe-off; normal R swing- through by day 10.
- Increased postural control: BBS 43/56 by day 10.
- Improved right LE muscle force production capacity: Upright motor control test - knee ext moderate, knee flex weak. Maintain isometric muscle force measured by the MRC-scale. Both by day 15.
Environmental factors
- Hours available for individual PT intervention sessions: 9 x 45 min.
- Total duration of rehabilitation period is 17 days in July/August.
- Inpatient rehabilitation centre with a large recreation & garden area with small hills and different surfaces (e.g. concrete, rocks, wooden floorboards, grass, sand), large well-equipped exercise hall (including among others steps, parallel bars, plints), well-equipped gym.
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; NPIP = non-patient identified problem; OT = occupational therapist; ROM = range of motion; PSCQ = patient-specific complain questionnaire; VAS = Visual Analogue Scale; MSWS-12 = Multiple Sclerosis Walking Scale - 12; 25FWT = 25-foot (7.62m) Walk Test; w/ = with; SF-36 PCS (physical component summary score); SF-36 MCS (mental component summary score); OGA = Observational Gait Analysis; BBS = Berg Balance Scale; MRC-scale = Medical Research Council Scale; MAS = Modified Ashworth Scale; R = right; L = left; UMCT = Upright Motor Control Test.
As Maya does not have individualised physical therapy at her home environment, training plan is made to encourage Maya continue being physically active after the rehabilitation period. The aim of the plan is to maintain / improve her physical capacity (see P5) and to ensure that Maya and her husband have adequate knowledge of MS and understand the consequences:
- Aerobic exercise (e.g. walking, cross-trainer, swimming): 3 x week, 15-30 minutes as tolerated, intensity as tolerated
- Muscle strength: core stability, hip adbuctors, knee extension, back extension 2-3 x week, 2-3 x 12 -15 rep as tolerated, intensity as tolerated (body weight or ankle weights)
- Balance exercises: integrate into ADLs, daily as tolerated.
- Separate information sessions for Maya and her husband and the whole family.
Rationale & evidence
- Task- and context-specific motor learning principles were adapted in the interventions (Morris et al. 2002, Pearson et al. 2004; Shumway-Cook et al. 2012).
- Problem - specific activities and tasks that provide a challenge for the multiple systems involved in walking were included. This approach seems to be more effective that exercises targeting a single system. The activities and tasks were systematically progressed from easy to challenging (Shumway-Cook et al. 2012).
- Try-out periods of dynamic ankle supports were included with the aim to assist ankle dorsiflexion and to prevent knee hyperextension (NICE 2003, Shumway-Cook et al. 2012).
- Core stability exercises were included for Maya to learn strategies to control her trunk when walking (Shumway-Cook et al. 2012).
- Prevention plan: A comprehensive plan was created in an attempt to guide Maya in remaining physically active. Intensive exercise programs do not influence the progression of MS or cause exacerbations (Beckerman et al. 2010).
Reassessment
Actions to take
Review reassessment findings
- Review the progress notes and reassessment findings in the Case details below.
- Report the reassessment findings for the goals and testing & predictive criteria.
Canvas - 'Problem tracking' sheet - 'Progress / discharge' column: note the findings of functional measures and testing & predictive criteria.
Canvas exampleReassess existing problems
- Have the HOAC II - Part 2 algorithm in hand. (If you're still missing it, you can get it here.)
- Follow the 'Reassessment of Existing Problems'.
Reassess anticipated problems
- Have the HOAC II - Part 2 algorithm in hand. (If you're still missing it, you can get it here.)
- Follow the 'Reassessment of Anticipated Problems'.
Reflect, review & continue
- Click 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as a foundation for the next section.
- Continue to the summary.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Great work - your PT expertise has just gone up another notch!
Case details
Progress notes
- At the end of the rehabilitation period Maya was consciously able to integrate the trained components into her gait pattern. However, this required concentration and when Maya was tired, the quality of her gait deteriorated.
- Maya began to prefer walking with two crutches to aid her to keep symmetric gait pattern. She found the dynamic ankle support extremely helpful; it made walking less tiring.
Reassessment findings
- PSCQ walking outside with 1 crutch + dynamic ankle support: VAS 80/100mm; distance 112m; time 3:53min
- MSWS - 12: 48/60
- 25FWT 1 crutch + dynamic ankle support: 12.7 sec
- 25FWT 2 crutches + dynamic ankle support: 9.8 sec
- PSCQ (walking max distance): VAS (low back pain) 0/100mm
- OGA: weight shifts completely to R, slight Trendelenburg, no hip circumduction, no knee hyperextension. Trunk remains in midline.
- BBS 46/56. Specific items: sit to stand 4; stand to sit 4; transfers 4; standing 2 min 4; sitting 4; standing feet together 2 (can place feet together & stand 25 sec); standing eyes closed 4; functional reach 4 (27cm); look over shoulder 4; slipper reach 4; 360 degree turn 2 (R 14.8 sec, L 6.7 sec); stool touch 2 (can complete 4 steps without help); tandem stand 3 (30 sec, R foot in front); one-foot stand 1 (R 2.5 sec, L 15.3 sec).
- Upright motor control test: knee extension – moderate/weak (able to support body weight on R flexed knee for 2sec); knee flexion – weak (10 sec to complete 3 repetitions).
- Isometric force generation - MRC-scale: all R LE muscle groups ≤3/5, m. peroneus 1/5; all L LE muscle groups 4/5.
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; NPIP = non-patient identified problem; OT = occupational therapist; ROM = range of motion; PSCQ = patient-specific complain questionnaire; VAS = Visual Analogue Scale; MSWS-12 = Multiple Sclerosis Walking Scale - 12; 25FWT = 25-foot (7.62m) Walk Test; w/ = with; SF-36 PCS (physical component summary score); SF-36 MCS (mental component summary score); OGA = Observational Gait Analysis; BBS = Berg Balance Scale; MRC-scale = Medical Research Council Scale; MAS = Modified Ashworth Scale; R = right; L = left; UMCT = Upright Motor Control Test.
At the end of the rehabilitation period it was clear that Maya was going to get the dynamic ankle support. The reassessment was done with Maya wearing the dynamic ankle support to reflect her functional capacity.
Reassessment of existing problems
Have the goals been met? PSCQ - VAS yes; distance yes; 25FWT - 1 crutch: no; 25FWT - 2 crutches: yes.
- PSCQ and 25FWT with two crutches: Measurements indicate that testing criteria have been met. Based on the measurements, the credibility of the hypotheses seem to be acceptable.
- 25FWT 1 crutch:
- Do measurements indicate if the testing criteria have been met? yes
- Is each hypothesis appropriate and are the testing criteria correct for that hypothesis? yes
- No testing criteria was considered to need revision.
Reassessment of the anticipated problems
The anticipated problems were not reassessed at the end of the 17 day rehabilitation rehabilitation period. The reassessment will be done by her personal PT in her home environment in 3 months time or in the next rehabilitation period in 6-12 months. The results serve as baseline details for individual physical therapy Maya will begin to receive at home.
Rationale & evidence
The quality of Maya's gait improved considerably during the 17-days. Yet, good quality gait was automated and required a lot of concentration. Maya began to prefer walking with two crutches and this may reflect on the faster walking speed with two crutches in the 25FWT.
Summary
- Well done! Now what? maybe get a cup of tea, rest, digest... and be sure to come back for more later!
Now you have got the hang of the HOAC II way of clinical reasoning. Very nice! You may want to check out the complete HOAC II algorithm (part 1 and part 2) and grasp the full picture of the process you have gone through. If you would still like to brush up your knowledge of the HOAC II, the article by Rothstein et al. (2003) has a lot of nice information. Otherwise, you could just continue developing your clinical reasoning skills with the different cases here on getptsmart.com and build up your knowledge of the HOAC II as you go.
Disclaimer
This case study is based on a real patient case. However, the name and personal details have been changed and some case details modified.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}