
Introduction
- Click on menu point "1" (in the menu above or below) when you're all set!
- Pay attention to these sticky notes. They'll help you here and there throughout the case.
Wait a sec. Is your toolbox filled? If not, then...
Download the Algorithm Download the Canvas
You may also want to watch this short introduction video.
Paul is an 80 year old male who suffered from a recurrent left hemisphere CVA one year ago. Paul was referred to physical therapy in his home environment by his treating general physician Dr. H. B. The aim of the referral is to advance ambulation and transfers.
Disclaimer
The foundation of the case study is based on a real patient case. However, the content is much simplified to maintain focus on learning the very basics of the HOAC II way of clinical reasoning. We do not provide you with information on the pathology but if you feel like brushing up your knowledge, browsing through PubMed Health may come handy.
Initial data (referral & medical record)
Actions to take
Activate your knowledge base
- You already received information on the patient's pathology, age and gender in the introduction. Take a few moments to hypothesise in your mind on the types of problems you expect the patient to have and what factors may cause them. You could base your ideas on knowledge or previous experience.
- Once you are ready, continue to the next step of the actions to take: 'Review the patient demographics'.
Review patient demographics
- Review the case details below.
- Record the case details in your paper version of the Canvas as advised in the Italics below.
- It's a good idea to check the yellow sticky notes next to the case details - they'll help you throughout the case.
Canvas - 'Initial Data' sheet: fill in the boxes on the top part of the sheet.
Canvas examplePrepare data collection
- Prepare for a hypothesis-driven data collection. It is a good idea to use the ICF Core Sets as the basis. Download the applicable Core Sets here.
- Begin to hypothesise on what activity limitations & participation restrictions the patient most likely has.
- Begin to hypothesise on probable underlying impairments and contextual factors.
- Record the guidelines and other evidence you plan to use in the case.
ICF Core Set - select the domains most relevant for the case.
Canvas - 'Initial Data' sheet - 'Guidelines, evidence & remarks' box: make relevant notes.
Reflect, review & continue
- Read the 'Solution' and click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 2.
Case details
Paul B. is an 80 year old male with right sided hemiparesis after a recurrent left hemisphere type CVA one year ago. Paul was referred to physical therapy in his home environment by his treating general physician Dr. H. B. The aim of the referral is to advance ambulation and transfers.
Basic information & medical history
Paul's first CVA occurred after a heart valve replacement six years back. He recovered without residual limitations or impairments from his first CVA. No other relevant past medical history.
Rehabilitation programme
Paul has three 40-60 minute long physical therapy sessions available on a weekly basis for as long as deemed necessary to reach the specified goals. He also has continuous weekly occupational therapy appointments.
Solution, rationale & evidence
Solution
Based on the problem areas of ambulation and transfers, the following categories of the ICF core set for stroke are selected for further investigation:
- b110 Consciousness functions
- b114 Orientation functions
- b167 Mental functions of language
- b730 Muscle power functions
- b735 Muscle tone functions
- b740 Muscle endurance functions
- b750 Motor reflex functions
- b755 Involuntary movement reaction functions
- b760 Control of voluntary movement functions
- b770 Gait pattern functions
- d450 Walking
- d460 Moving around in different locations
- d465 Moving around using equipment
- d530 Toileting
- e210 Physical geography
- e310 Immediate family
Rationale & evidence
The initial hypotheses, expressed as ICF categories above, are based on the KNGF guidelines (Peppen et al. 2004) and Shumway-Cook et al. (2012).
Interview & Problem list
Actions to take
Review collected data
- Review the data collected in the interview and informal observation from the Case details below.
- Record the collected data.
Canvas - 'Initial Data' sheet -'Interview & informal observation' box: Note the data in your preferred way.
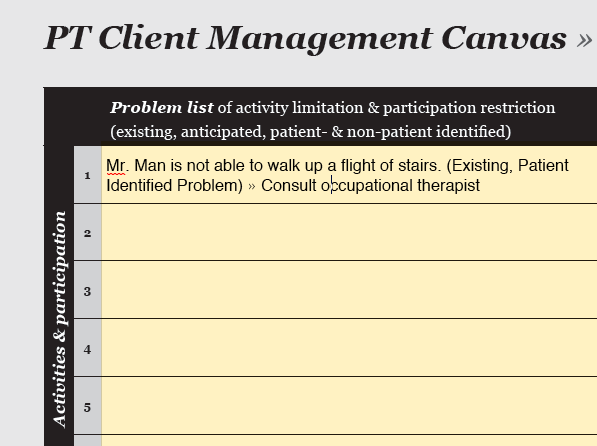
Canvas exampleGenerate existing problem list
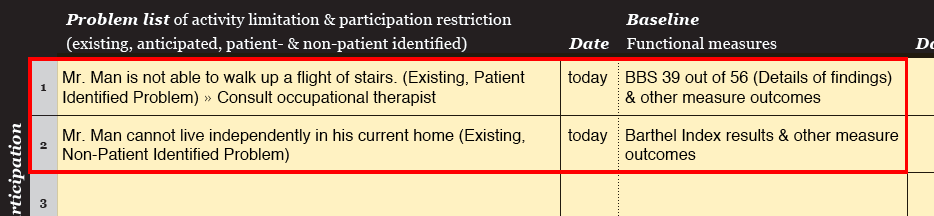
- Describe the existing Patient-Identified Problems (PIPs) in patient-orientated terms.
- In some cases you may already identify existing non-PIPs (NPIPs).
- Notice that in cases where the patient is unable to communicate, the problem list consists only of NPIPs.
Canvas - 'Problem Tracking' sheet - 'Problem list': Note all problems.
Generate anticipated problem list
- Describe any anticipated Patient-Identified Problems (PIPs) in patient-orientated terms.
- In some cases you may already identify anticipated non-PIPs (NPIPs).
- Notice that in cases where the patient is unable to communicate, the problem list consists only of NPIPs.
Canvas - 'Problem Tracking' sheet - 'Problem list': Note all problems.
Hypothesise on underlying factors
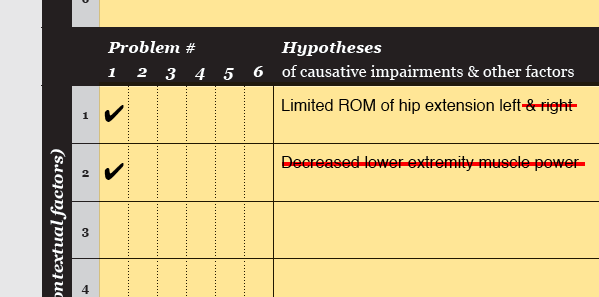
- Hypothesise on the impairments (and Contextual factors) underlying each problem.
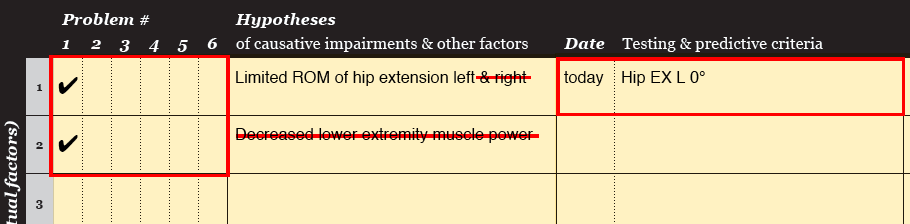
Canvas - 'Problem tracking' sheet - 'Hypotheses' column: list the causative factors and tick the Problem # they are related to.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 3.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Keep it up! You're just starting to get your clinical reasoning skills up to speed!
- Hypothesising on the underlying factors is super important. Those ideas form the basis of the whole case. So get your brain cells fired and working!
Case details
Review of activity & participation
Status quo
Paul reports that he feels unsafe during rollator aided ambulation in his home. He also notes that he cannot independently transfer from his wheelchair to a toilet and back.
His wife adds that she thinks he is unsafe when ascending or descending the seven steps to his garden without support.
Ambulation, transfer, fall & balance history
Paul ambulates with a wheelchair and with a rollator in his home. He reports one fall from two weeks ago. He fell backwards with his rollator in his carpeted and dim hallway. Unable to recall further details of possible reasons, he states that he may have tripped over his own foot. Paul did not experience any injuries with this fall. After the fall he needed help from his partner to raise from the floor.
He reports no further falls or difficulties with transfers besides the one mentioned above.
Pre morbid status
Paul reports no previous limitations or restrictions. He was fully independent in his daily life. After Paul retired from medical engineering his daily activities consisted of garden and household work, and frequent walks with his partner.
Review of environmental factors
Paul lives with his healthy and supportive partner in a level home on the ground floor. His partner is available for most parts of the day. A set of seven steps lead to the entrance of Paul’s home and to his garden. His garden steps have hand rails on both sides. His bathroom is too narrow to accommodate rollator aided ambulation.
Care
He receives home care for personal hygiene on daily basis.
Intervention history
Paul was admitted to stroke rehabilitation for a period of about eight weeks starting two week after his stroke. Following the rehabilitation program, he was treated by home based physical and occupational therapy three times 20 minutes each per week. He reports that his previous physical therapy mainly included gait training and upper extremity mobilization. The occupational therapist works on upper extremity function with Paul.
Review of personal factors
Paul is extremely motivated and ambitious to recover and appears to have a positive attitude. He does not consume tobacco or alcohol.
Review of body functions & structures
Past medical history
Aside from the previously mentioned first CVA, Paul reports a bilateral hernia inguinale from his 40s. He also reports to have mildly impaired hearing.
Family history
Paul reports no relevant family history.
Informal observation & impression
Paul appears to have mild cognitive impairments, but he shows no difficulties responding accurately to short questions.
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); NPIP = non-patient identified problem; ROM = range of motion.
Please review the solution on page 2 in the Canvas on the right.
Rationale & evidence
The problem list and hypotheses of causative impairments are based on the KNGF guidelines (Peppen et al. 2004) and Shumway-Cook et al. (2012).
Examination strategy
Actions to take
Formulate examination strategy
- Review the Case details below.
- Formulate an examination strategy to assess the extend of the identified problems. Use tests and measurements at activity & participation level.
- Formulate an examination strategy to assess if the hypothesised underlying factors are correct. Use tests & measures mostly at body functions & structures level.
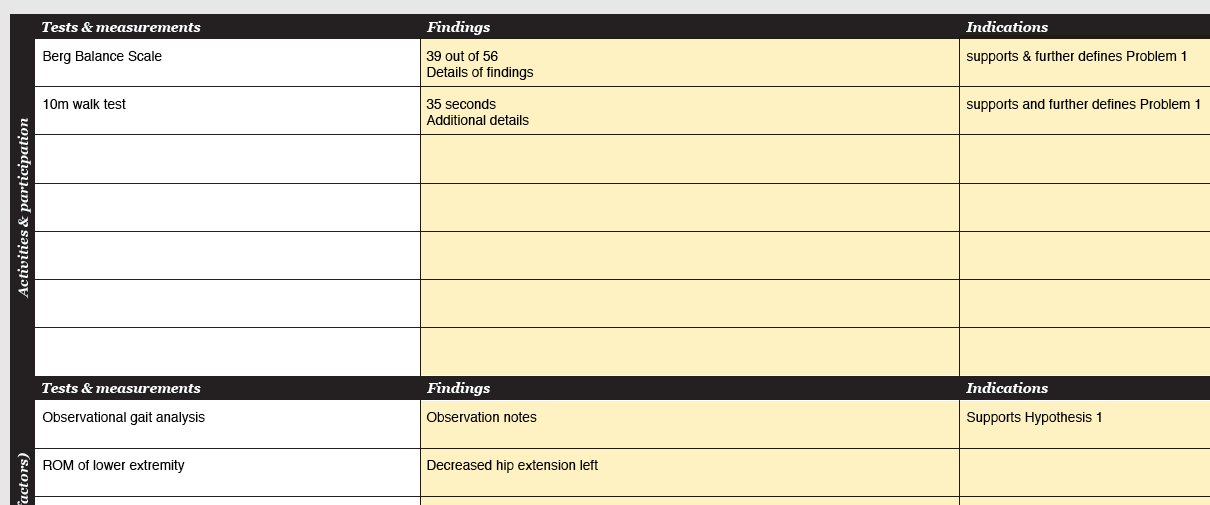
Canvas - 'Examination' sheet - 'Tests & measurements': note the tests & measurements.
Canvas exampleSeek consultation if needed
- When it is not possible to generate an examination strategy for a problem or an underlying factor, seek consultation from other health care professionals.
Canvas - 'Problem tracking' sheet - 'Problem list' / 'Hypotheses' columns: Note the need for consultation next to the relevant problem / causative factor.
Canvas exampleReflect, review & continue
- Click 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 4.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Are you already giving all those brain cells a good work out? "No ideas of causation, no examination strategy..."
Case details
Identified problems (P)
- P1: Paul feels unsafe during rollator aided ambulation in his home (E)
- P2: Paul's wive thinks that he is unsafe when ascending or descending the seven steps to his garden without support (NPIP - E)
- P3: Paul cannot independently transfer from his wheelchair to a toilet and back (E)
- P4: Paul is expected not to be able to perform ADLs, such as walking in home and garden, for prolonged periods of time (NPIP - A)
Hypothesised causations (H)
- H1: P1, P2 & P3 are related to impaired motor components of the balance strategy
- H2: P1, P2 & P3 are related to impaired sensory components of the balance strategy
- H3: P1, P2 & P3 are related to lower extremity paresis
- H4: P1, P2 & P3 are related to impaired lower extremity ROM
- H5: P1, P2 & P3 are related to abnormal tonus in lower extremity
- H6: P1, P2 & P3 are related to abnormal synergies in the lower extremities
- H7: P4 is related to general physical deconditioning
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: BBS = Berg Balance Scale; TUG = Timed Up and Go Test; mCTSIB = modified Clinical Test For Sensory Interaction In Balance; P-ROM = Passive range of motion; MAS = Modified Ashworth Scale; MRC = Medical Research Council; A-ROM = Active range of motion; P = Problem; H = Hypothesis.
Please review the solution on page 2 in the Canvas on the right.
Rationale & evidence
Activities & participation
- Functional measures are set according to Peppen et al. 2004 and/or Shumway-Cook et al. 2012
Body functions & structures
- Balance is divided into motor and sensory components based on Shumway-Cook et al. (2012)
- Alignment: for assessment of static balance control
- Voluntary sway forward, backward, side-to-side: for observation of anticipatory balance control
- Nudge test: for assessment of reactive balance control
- Modified Test of Sensory Interaction and Balance (mCTSIB): for assessment of sensory components of balance control
- Manual isometric muscle testing using the Medical Research Council (MRC) - scale: for assessment of muscle force generation capacity
- Passive range of motion (PROM): for assessment of passive range of motion
- Modified Ashworth Scale (MAS): for assessment of muscle tone
- Cardiovascular capacity: measured on home ergometer with resistance settings of 1 to 10, no details regarding Watts, etc. were available
Note
The real case included additional measures assessing the quality of performance, e.g. Observational Gait Analysis (Schumway-Cook et al. 2012). We chose to exclude this data for sake of simplification.
Examination findings
Actions to take
Review & analyse findings
- Review the examination findings from the Case details below.
- Record the examination findings. Aim to include only the most important findings in the Canvas.
- Analyse whether the findings support or refute the identified problems and hypothesised underlying factors.
Canvas - 'Examination' sheet - 'Findings' column: record the findings.
Canvas - 'Examination' sheet - 'Indications' column: note whether the findings support or refute any of the identified problems and hypothesised underlying factors.
Refine underlying factors
- Refine the hypothesised underlying factors and cross-out the refuted ones.
- (When the findings do not provide enough information for you to accept or refute the hypothesised underlying factors, carry out additional examination procedures following the same procedure as outlined in the 'Examination strategy'.)
Canvas - 'Problem Tracking' sheet - 'Hypotheses' column: refine /cross-out hypothesised underlying factors.
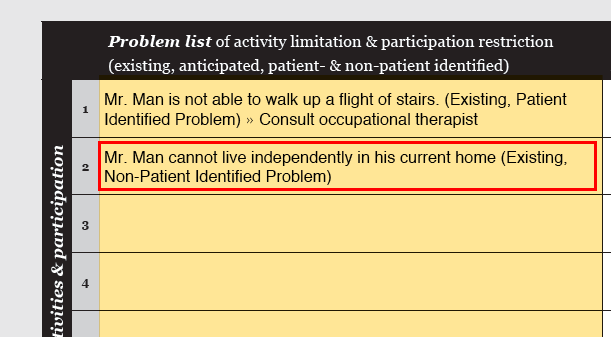
Add NPIPs
- Often (additional) Non-Patient Identified Problems (NPIPs) are identified in the examination. Now that the examination is completed, all NPIPs should have been identified. Note whether the NPIPs are existing or anticipated.
Canvas - 'Problem tracking' sheet - 'Problem list' column: add NPIPs.
Canvas exampleHypotheses & rationale
- From this point on the accepted underlying factors are called hypotheses. The reasons as to why an anticipated problem is justified is called rationale.
- Check that each existing problem is linked to hypotheses. Note the baseline measure of the underlying impairments.
- Check that you have identified rationale for each anticipated problem.
- If you decide to consult another health care professional, document the reason.
Canvas - 'Problem Tracking' sheet - 'Hypotheses' column: Link all problems to hypotheses or rationale. Elaborate on the rationale e.g. on the backside of the problem tracking sheet.
Canvas - 'Problem Tracking' sheet - 'Baseline' column: Note the baseline of the examination measurements for each hypothesis.
Refine problem list
- Identify problems that should be treated by other health professionals, remove them from the problem list and make a referral.
- Identify problems that cannot be fully resolved and modify the problem statement.
- Any changes in the PIPs should only be made after a discussion with the patient. Notice that after this step PIPs and NPIPs are treated the same way.
- Note the baseline measures for all retained problems.
Canvas - 'Problem Tracking' sheet - 'Problem list': Refine the problems if necessary.
Canvas - 'Problem Tracking' sheet - 'Baseline' column: Note the baseline measures for each problem.
Reflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 5.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- The clinical reasoning steps in this section very much relate to one another and help you work toward the final problem list and hypothesis & rationale list. Precise and specific lists will make the rest of the clinical reasoning process flow by!
Case details
Activities & participation
- BBS: Total score: 31; 1.) 2; 2.) 4; 3.) 4; 4.) 3 w/ hand use; 5.) 1 no control stand to sit on chair w/o arm rests, needed assistance; 6.) 3; 7.) 3; 8.) 3; 9.) 3; 10.) 4; 11.) 0 PT caught a fall; 12.) 0; 13.) 0; 14.) 1
- TUG: Aids: rollator; Time: 1:40; Observation: increased time for transfers & hand prep, decreased time for ambulation; Fatigue VAS 7.5 / 10cm
- Upright motor control test: A: weak; B: strong
Body functions & structures
- Alignment: Alignment in sit & stand: shifted to the left; Ambulation: trunk & hip flexion
- Movement strategies: Self-initiated: Voluntary sway: Uses hip strategy; has difficulty shifting weight to the right
- Movement strategies: Reactive: Nudge test: Small perturbations: less, but apparent DF R; Large perturbations: NOT TESTED
- Movement strategies: Anticipatory: Maintains balance with BBS arm reach test @
- Modified CTSIB: Firm surface: open eyes >30s, closed eyes >30s; Foam surface: open eyes >30s, closed eyes 10s, >30s
- Synergies / fractination: R lower limb reveals no synergies in seated position during strength & A-ROM
- Strength - isometric: Position: seated w/ 90° Hip/Knee FL; Hip R FL 3+, EX 4; Knee R 4-; Ankle R DF 1
- MAS: Ankle Plantar Flexors 1 (w/clonus); Knee Flexors 1
- P-ROM: no findings
- Cardiovascular capacity (on home bike ergometer): load level 2/10 biking for 10 minutes » Rate of perceived exertion (RPE) Borg scale (6-20) 15
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: BBS = Berg Balance Scale; TUG = Timed Up and Go Test; mCTSIB = modified Clinical Test For Sensory Interaction In Balance; P-ROM = Passive range of motion; MAS = Modified Ashworth Scale; MRC = Medical Research Council; A-ROM = Active range of motion; P = Problem; H = Hypothesis.
Please review the solution on page 2 & 3 in the Canvas on the right.
Rationale & evidence
Rationale for the anticipated problem of physical deconditioning (P4) is based on Peppen et al. 2004; Pang et al. 2006; Michael et al. 2009; Saunders et al. 2009; National stroke foundation 2010.
Goals
Actions to take
Specify existing problems
- Review the Case details below.
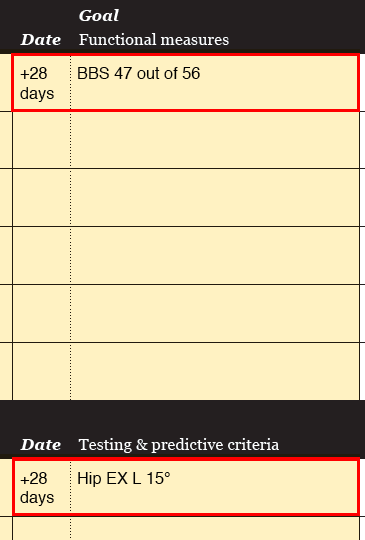
- Establish goals for all problems by setting a target level for the functional measures. Determine when you can expect the patient to meet the goal and set dates of reassessment accordingly.
- Establish testing criteria for each hypothesis. Determine when you can expect the patient to meet the testing criteria and set dates of reassessment accordingly.
Canvas - 'Problem Tracking' sheet - Goal column: Note goals for functional measures and testing criteria. Note dates of reassessment.
Canvas exampleSpecify anticipated problems
- Establish predictive criteria for each anticipated problem. Determine when the predictive criteria should be achieved for the problem to be eliminated. Set dates of reassessment accordingly.
Canvas - 'Problem Tracking' sheet - Goal column: Note goals for functional measures and predicitive criteria. Note dates of reassessment.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 6.
Download the filled Canvas to catch up to the current step of the case
Filled CanvasWhen you follow the points in the 'Actions-to-take' list, you will automatically have the basis of your SMART- goals on the Canvas. Smart, isn't it!
Despite of the smart Canvas, writing SMART-goals can be a little tricky sometimes. You could check this practical guide (Bovend'Eerdt et al. 2009) for extra advice. Step 1 is about writing SMART-goals.
Case details
There are no new case details in this section. However, keep this section of the interview in mind when setting your goals: "Paul is extremely motivated and ambitious to recover and appears to have a positive attitude."
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: BBS = Berg Balance Scale; TUG = Timed Up and Go Test; mCTSIB = modified Clinical Test For Sensory Interaction In Balance; P-ROM = Passive range of motion; MAS = Modified Ashworth Scale; MRC = Medical Research Council; A-ROM = Active range of motion; P = Problem; H = Hypothesis; A = Alignment; VS = Voluntary sway; R = Right; LE = Lower extremity; Sym. - Symmetry; Decr = Decreased.
Please review the solution on page 2 in the Canvas on the right.
Rationale & evidence
- P1 — Despite Paul’s age (80), he has a good chance to recover a high ambulatory function based on the function of his paretic leg (synergies and strength), the available support and his motivation (Peppen et al. 2004). Note: The real case included a short-term and long-term goal. The long-term goal (with a time of completion set to 5 weeks) included Paul walking safely with one crutch.
- P2 — Peppen et al. (2004) and Shumway-Cook et al. (2012) support necessary adaptation on functional and impairment level.
- P3 — See Monger et al. 2002 for a detailed rational. Note: the real case included a short-term and long-term goal. This case only features the long-term (outcome) goal.
- P4 – See Peppen et al. 2004; Palmer-McLean et al. 2009; National stroke foundation 2010 for a detailed rational.
Intervention strategy
Actions to take
Plan intervention strategy
- Review the Case details below.
- Plan the intervention strategy. Briefly explain why the strategy should lead to changes in testing & predictive criteria.
- Consider the environmental factors given in the Case details when planning the interventions.
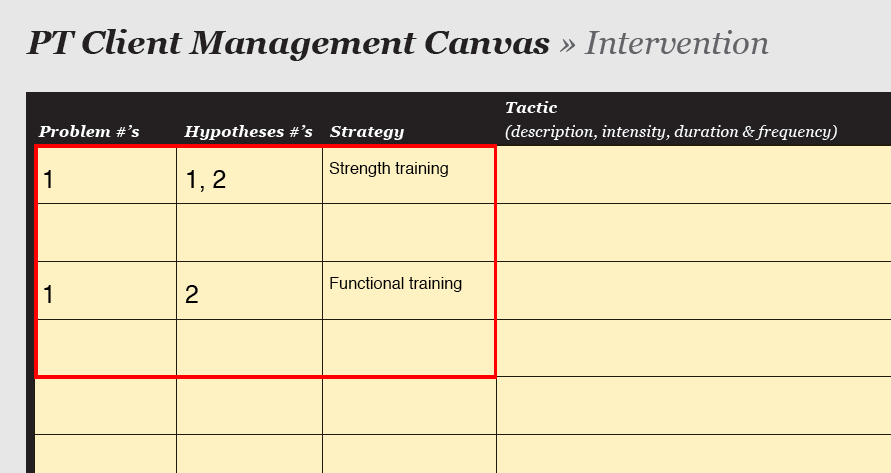
Canvas - 'Intervention' sheet - 'Strategy': Note the strategy and (very) brief reasoning for it.
Canvas examplePlan tactics
- Plan the tactics and relate each tactic to a hypothesis.
- Specify progression.
- Specify the implementer.
Canvas - 'Intervention' sheet - 'Tactics', 'Progression & Remarks', 'Implementer': Note the relevant information.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 7.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- "Success comes from knowing that you did your best to become the best that you are capable of becoming." (John Wooden) :-)
Case details
Goals
- P1 — Paul can safely ambulate with a rollator in his home. BBS >45; TUG
- P2 — Paul can safely ascent and descent the seven steps to his garden. BBS >45; UMCT - A: moderate; B: strong
- P3 — Paul can independently transfer from his wheelchair to a toilet and back. BBS >45; TUG
- P4 – Paul can perform ADLs, such as walking in his home and garden, without early fatigue. TUG fatigue VAS 5 / 10cm
Testing criteria
- H1 — Impaired motor components of the balance strategy. Alignment: Frontal symmetry; upright posture; Voluntary sway: Decreased hip strategy; able to load right lower extremity; Nudge test: Increase in DF R; BBS arm reach: @ > 10 inches
- H3 — Paresis of R Hip FL; R Knee Fl/EX & R Ankle DF. Hip R FL >4; Knee R >4; Ankle DF >2
- H5 — Lower extremity spasticity & abnormal tonus. no change
- H7 – Load level 2/10 biking for 10 minutes » RPE Borg scale (6-20) 13
Environmental factors
- Paul has three 40-60 minute long physical therapy sessions available on a weekly basis for as long as deemed necessary to reach the specified goals. He also has continuous weekly occupational therapy appointments.
Solution, rationale & evidence
Solution
Please review the solution on page 4 in the Canvas on the right.
Rationale & evidence
The choice for the tactics was based on the following rationale & evidence:
- Gait pattern - whole task: Task & context specific motor learning (Peppen et al. 2004, National stroke foundation 2010, Shumway-Cook et al. 2012)
- Gait pattern - part practice: Kahn et al. 2009; National stroke foundation 2010, Shumway-Cook et al. 2012
- Gait - obstacle navigation: Task & context specific motor learning (Peppen et al. 2004, Shumway-Cook et al. 2012)
- Sit to stand to sit: Task & context specific motor learning (Peppen et al. 2004); Monger et al. 2002; Ada et al. 2006; Palmer-McLean et al. 2009 for exercise specifications; National stroke foundation 2010
- Stair climbing: Task & context specific motor learning (Peppen et al. 2004)
- Single leg stance: Shumway-Cook et al. 2012; Lubetzky-Vilnai et al. 2010
- Voluntary sway: Shumway-Cook et al. 2012; Lubetzky-Vilnai et al. 2010
- High squats: Monger et al. 2002; Ada et al. 2006; Palmer-McLean et al. 2009 for exercise specifications
- High steps: Ada et al. 2006
- Ergometer: Palmer-McLean et al. 2009; Saunders et al. 2009; National stroke foundation 2010
Reassessment
Actions to take
Review reassessment findings
- Review the progress notes and reassessment findings in the Case details below.
- Report the reassessment findings for the goals and testing & predictive criteria.
Canvas - 'Problem tracking' sheet - 'Progress / discharge' column: note the findings of functional measures and testing & predictive criteria.
Canvas exampleReassess existing problems
- Have the HOAC II - Part 2 algorithm in hand. (If you're still missing it, you can get it here.)
- Follow the 'Reassessment of Existing Problems'.
Reassess anticipated problems
- Have the HOAC II - Part 2 algorithm in hand. (If you're still missing it, you can get it here.)
- Follow the 'Reassessment of Anticipated Problems'.
Reflect, review & continue
- Click 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as a foundation for the next section.
- Continue to the summary.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Great work - your PT expertise has just gone up another notch!
Case details
Reassessment findings - problems & functional measures
- P1 — Paul feels safe when ambulating with a rollator in his home. BBS 37; TUG 0:55; UMCT - A: moderate; B: strong
- P2 — Paul feels safe while ascending and descending the seven steps to his garden. BBS 37; UMCT - A: moderate; B: strong
- P3 — Paul can independently transfer from his wheelchair to a toilet and back. BBS 37; TUG 0:55
- P4 – Paul can perform his ADLs, such as walking in his home and garden, without early fatigue. TUG fatigue VAS 6 / 10cm
Reassessment findings - testing criteria
- H1 — Impaired motor components of the balance strategy. Alignment: Frontal sym.; upright posture; Voluntary sway: Decreased hip strategy; can load R LE; Nudge test: mild increase in DF R; BBS arm reach: @ 12 inches
- H3 — Paresis of R Hip FL; R Knee Fl/EX & R Ankle DF. Hip R FL 4; Knee R FL 4-, EX 4+; Ankle DF 4-
- H 5 — Lower extremity spasticity & abnormal tonus. no change
- H7 – Load level 2/10 biking for 10 minutes » RPE Borg scale (6-20) 12
Solution, rationale & evidence
Solution
Reassessment of the problem based on HOAC II part 2 (Existing & anticipated problems)
All goals have been achieved. The functional measures and hypothesised testing criteria are only partially credible. A progress can be seen in all aspects, however, the goals were reached without achievement of some of the related functional measures and testing criteria. It is hypothesised that increased strength and balance have had a significant effect on the attainment of the goals, however, the individual outcome measures were unnecessarily high.
Summary
- Well done! Now what? maybe get a cup of tea, rest, digest... and be sure to come back for more later!
Now you have got the hang of the basics of the HOAC II way of clinical reasoning. Very nice! You may want to check out the complete HOAC II algorithm (part 1 and part 2) and grasp the full picture of the process you have gone through. You might feel the need to brush up your knowledge of the HOAC II - the article by Rothstein et al. (2003) has a lot of nice information. Otherwise, you could just continue developing your clinical reasoning skills with a medium level case here on getptsmart.com and build up your knowledge of the HOAC II as you go.
Disclaimer
This case study is based on a real patient case. However, the name and personal details have been changed and the case was moderately modified and simplified.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}