
Introduction
- Click on menu point "1" (in the menu above or below) when you're all set!
- Pay attention to these sticky notes. They'll help you here and there throughout the case.
Wait a sec. Is your toolbox filled? If not, then...
Download the Algorithm Download the Canvas
You may also want to watch this short introduction video.
This case study is about Anna, a 35-year-old lady diagnosed with Multiple Sclerosis 10 years ago who has problems with her balance. The content is set at easy level so the case is a nice way to start getting acquainted with the HOAC II way of clinical reasoning.
Disclaimer
The foundation of this case study is based on a real patient case. However, the content is much simplified to maintain focus on the learning experience. We don’t provide information on the pathology in the cases but if you feel like brushing up your knowledge of MS, browsing through PubMed Health and our reference list may come handy.
Initial data (referral & medical record)
Actions to take
Activate your knowledge base
- You already received information on the patient's pathology, age and gender in the introduction. Take a few moments to hypothesise in your mind on the types of problems you expect the patient to have and what factors may cause them. You could base your ideas on knowledge or previous experience.
- Once you are ready, continue to the next step of the actions to take: 'Review the patient demographics'.
Review patient demographics
- Review the case details below.
- Record the case details in your paper version of the Canvas as advised in the Italics below.
- It's a good idea to check the yellow sticky notes next to the case details - they'll help you throughout the case.
Canvas - 'Initial Data' sheet: fill in the boxes on the top part of the sheet.
Canvas examplePrepare data collection
- Prepare for a hypothesis-driven data collection. It is a good idea to use the ICF Core Sets as the basis. Download the applicable Core Sets here.
- Begin to hypothesise on what activity limitations & participation restrictions the patient most likely has.
- Begin to hypothesise on probable underlying impairments and contextual factors.
- Record the guidelines and other evidence you plan to use in the case.
ICF Core Set - select the domains most relevant for the case.
Canvas - 'Initial Data' sheet - 'Guidelines, evidence & remarks' box: make relevant notes.
Reflect, review & continue
- Read the 'Solution' and click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 2.
- A brief and a comprehensive Core Set are available for MS. Check which one covers most aspects of functioning related to a balance problem.
- Need more explanation of the HOAC II terms or to refresh the ICF terms? Check the highlighted terms for definitions.
Case details
Patient demographics
Anna is a 35-year-old woman diagnosed with a relapsing-remitting form of multiple sclerosis 10 years ago. In the last six months Anna has had more problems with her standing balance in different activities at work. She has been referred for a 14-day multidisciplinary inpatient rehabilitation.
Referral & medical record information
Height 166cm, weight 65kg. Current medication n/a. No other significant past medical history.
Anna lives with her boyfriend and two dogs in a single-story house. Anna works three days a week as a primary school arts and handicrafts teacher.
Rehabilitation programme
Individual appointments have been scheduled with neurologist, physical therapist and occupational therapist.
Solution, rationale & evidence
Solution
The short ICF Core Set for MS does not include all relevant ICF categories for balance, therefore we use the comprehensive Core Set (accessed on 6 December 2011).
- b235 Vestibular functions
- b260 Proprioceptive function
- b265 Touch function
- b270 Sensory functions related to temperature and other stimuli
- b455 Exercise tolerance functions
- b710 Mobility of joint functions
- b730 Muscle power functions
- b735 Muscle tone functions
- b760 Control of voluntary movement functions
- d410 Changing basic body position
- d415 Maintaining a body position
- d455 Moving around
Rationale & evidence
Motor, sensory and perceptual components contribute to balance control (Shumway-Cook et al. 2012; see chapter 10).
Interview & Problem list
Actions to take
Review collected data
- Review the data collected in the interview and informal observation from the Case details below.
- Record the collected data.
Canvas - 'Initial Data' sheet -'Interview & informal observation' box: Note the data in your preferred way.
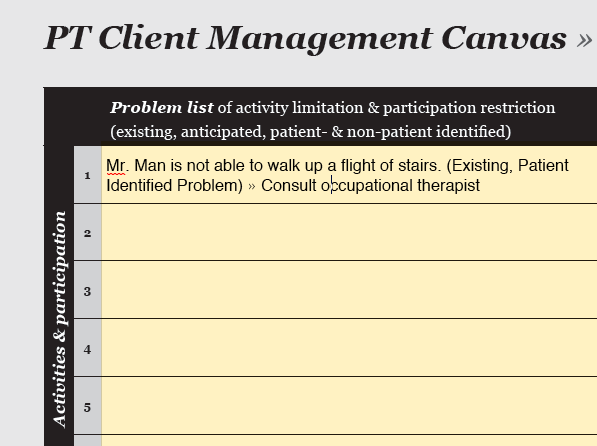
Canvas exampleGenerate existing problem list
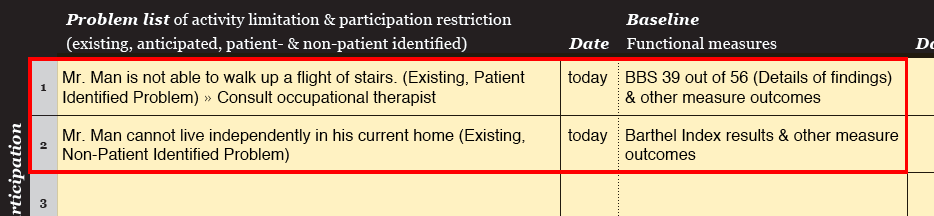
- Describe the existing Patient-Identified Problems (PIPs) in patient-orientated terms.
- In some cases you may already identify existing non-PIPs (NPIPs).
- Notice that in cases where the patient is unable to communicate, the problem list consists only of NPIPs.
Canvas - 'Problem Tracking' sheet - 'Problem list': Note all problems.
Generate anticipated problem list
- Describe any anticipated Patient-Identified Problems (PIPs) in patient-orientated terms.
- In some cases you may already identify anticipated non-PIPs (NPIPs).
- Notice that in cases where the patient is unable to communicate, the problem list consists only of NPIPs.
Canvas - 'Problem Tracking' sheet - 'Problem list': Note all problems.
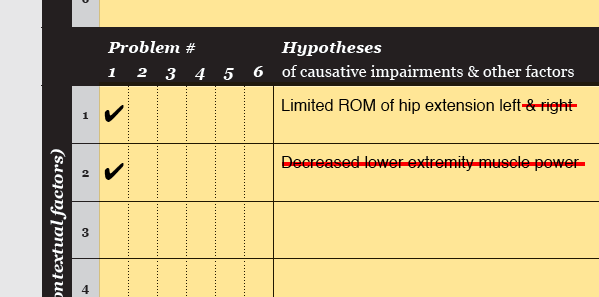
Hypothesise on underlying factors
- Hypothesise on the impairments (and Contextual factors) underlying each problem.
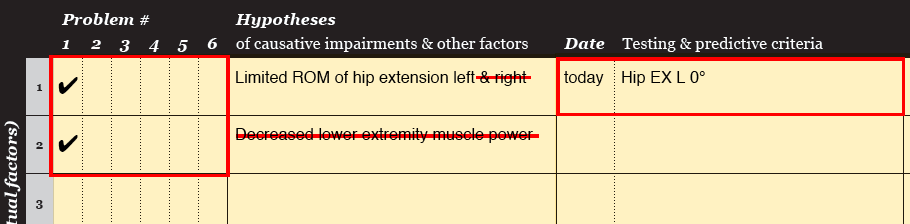
Canvas - 'Problem tracking' sheet - 'Hypotheses' column: list the causative factors and tick the Problem # they are related to.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 3.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Hypothesising on causation is super important. Those ideas form the basis of the whole case. In the next step you will formulate an examination strategy - which, well, can't exist without any ideas of causative factors...
- John Woods once said: "Failing to prepare is preparing to fail". Very true here!
Case details
Anna has experienced more difficulties with her balance in the last six months. The most challenging activities for Anna include reaching forward, picking up something from the floor, turning to look behind her shoulder or turning around quickly. Anna is a primary school arts and handicrafts teacher and needs to be confident in performing those tasks in a busy classroom environment. Anna has no history of falls.
Anna's favourite pastime is walking with her dogs. She walks approximately 2km daily, which is as far as Anna wants to walk. Anna does not have balance problems in walking. She wears a knee support on her right knee to prevent hyperextension. When she gets tired, Anna has to concentrate a lot in positioning her legs for instance when turning around. She often feels pins and needles in her feet, especially on the right, and always wears socks to keep her feet warm. Anna does not perceive fatigue as a big problem limiting her life.
Personal & environmental factors
Anna is very motivated and has good coping strategies. Anna works three days a week. At the moment she sees a physical therapist once in two weeks.
Expectations
"I want to be confident that I maintain my balance when I do activities that include reaching forward, picking up something from the floor, turning to look behind my shoulder or turning around quickly. Those are activities I continuously need to do in my job."
Informal observation
No apparent cognitive deficits.
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity.
Rationale & evidence
The list of causative factors is based on the motor, sensory and cognitive / perceptual components that contribute to balance control (Carr et al. 1998, Shumway-Cook et al. 2012).
Examination strategy
Actions to take
Formulate examination strategy
- Review the Case details below.
- Formulate an examination strategy to assess the extend of the identified problems. Use tests and measurements at activity & participation level.
- Formulate an examination strategy to assess if the hypothesised underlying factors are correct. Use tests & measures mostly at body functions & structures level.
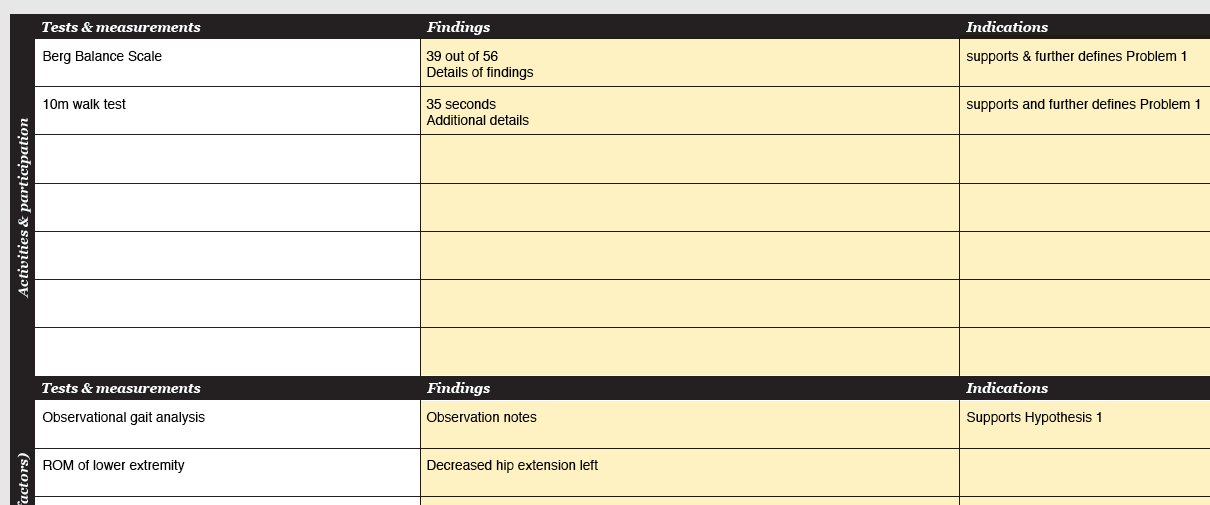
Canvas - 'Examination' sheet - 'Tests & measurements': note the tests & measurements.
Canvas exampleSeek consultation if needed
- When it is not possible to generate an examination strategy for a problem or an underlying factor, seek consultation from other health care professionals.
Canvas - 'Problem tracking' sheet - 'Problem list' / 'Hypotheses' columns: Note the need for consultation next to the relevant problem / causative factor.
Canvas exampleReflect, review & continue
- Click 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 4.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- "Don't let what you cannot do interfere with what you can do." (John Wooden) :-)
Case details
The following problems (P) were identified:
- P1 Lack of confidence in balance when reaching forward, picking up something from floor, looking over shoulder or turning around.
The following underlying factors were hypothesised (H):
- H1 Impaired motor component of balance strategy
- H2 Impaired sensory component of balance strategy
- H3 Impaired cognitive component of balance strategy
- H4 Decreased lower extremity force generation
- H5 Decreased lower extremity range of motion
- H6 Increased lower extremity muscle tone
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; BBS = Berg Balance Scale; ABC - scale = Activities-specific Balance Confidence - scale; CTSIB = Clinical test of Sensory Interaction and Balance; MRC - scale = Medical Research Council - scale; ROM = range of motion; MAS = Modified Ashworth Scale.
Rationale & evidence
Using a force platform (FP) would be the gold standard measure of balance and allow for precise measures of the centre of pressure (COP), which have been identified as important outcome measures of balance (Clark et al. 2010). As FPs are rarely available in clinical settings, subjective examination methods not requiring extra equipment were chosen in this case.
Activities & participation
- Berg Balance Scale (BBS) provides a standardised measure to assess task-specific complaints (Shumway-Cook et al. 2012), although it has a limited precision to detect small changes (Clark et al. 2010).
- Activities-specific Balance Confidence (ABC) - scale measures confidence in performing ADLs without falling. The ABC-scale is a 16-item questionnaire where 0 represents no confidence and 100 represents complete confidence in balance (Cattaneo et al. 2006).
Body functions & structures
- Alignment: for assessment of static balance control.
- Self-initiated sway forward, backward, side-to-side: for observation of anticipatory balance control. Cognitive tasks added to observe double-tasking.
- Nudge test: for assessment of reactive balance control (Shumway-Cook et al. 2012).
- Modified Test of Sensory Interaction and Balance (mCTSIB): for assessment of sensory components of balance control (Shumway-Cook et al. 2012).
- Manual isometric muscle testing using the Medical Research Council (MRC) - scale: for assessment of muscle force generation capacity.
- Passive range of motion (PROM): for assessment of passive range of motion.
- Modified Ashworth Scale (MAS): for assessment of muscle tone.
Assessment of the muscles around the ankle (m. tibialis anterior, m. gastrocnemius and m. soleus) is especially important in the examination of force generation capacity and ROM (Shumway-Cook et al. 2012).
- See Paltamaa (2008) and Paltamaa et al. (2008) for a discussion of the reliability, responsiveness and clinical usefulness of examination instruments in ambulatory persons with MS.
Examination findings
Actions to take
Review & analyse findings
- Review the examination findings from the Case details below.
- Record the examination findings. Aim to include only the most important findings in the Canvas.
- Analyse whether the findings support or refute the identified problems and hypothesised underlying factors.
Canvas - 'Examination' sheet - 'Findings' column: record the findings.
Canvas - 'Examination' sheet - 'Indications' column: note whether the findings support or refute any of the identified problems and hypothesised underlying factors.
Refine underlying factors
- Refine the hypothesised underlying factors and cross-out the refuted ones.
- (When the findings do not provide enough information for you to accept or refute the hypothesised underlying factors, carry out additional examination procedures following the same procedure as outlined in the 'Examination strategy'.)
Canvas - 'Problem Tracking' sheet - 'Hypotheses' column: refine /cross-out hypothesised underlying factors.
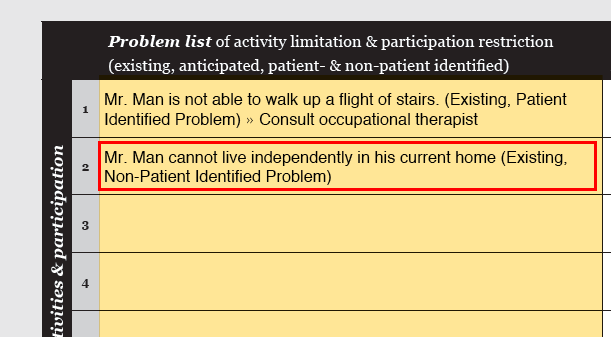
Add NPIPs
- Often (additional) Non-Patient Identified Problems (NPIPs) are identified in the examination. Now that the examination is completed, all NPIPs should have been identified. Note whether the NPIPs are existing or anticipated.
Canvas - 'Problem tracking' sheet - 'Problem list' column: add NPIPs.
Canvas exampleHypotheses & rationale
- From this point on the accepted underlying factors are called hypotheses. The reasons as to why an anticipated problem is justified is called rationale.
- Check that each existing problem is linked to hypotheses. Note the baseline measure of the underlying impairments.
- Check that you have identified rationale for each anticipated problem.
- If you decide to consult another health care professional, document the reason.
Canvas - 'Problem Tracking' sheet - 'Hypotheses' column: Link all problems to hypotheses or rationale. Elaborate on the rationale e.g. on the backside of the problem tracking sheet.
Canvas - 'Problem Tracking' sheet - 'Baseline' column: Note the baseline of the examination measurements for each hypothesis.
Refine problem list
- Identify problems that should be treated by other health professionals, remove them from the problem list and make a referral.
- Identify problems that cannot be fully resolved and modify the problem statement.
- Any changes in the PIPs should only be made after a discussion with the patient. Notice that after this step PIPs and NPIPs are treated the same way.
- Note the baseline measures for all retained problems.
Canvas - 'Problem Tracking' sheet - 'Problem list': Refine the problems if necessary.
Canvas - 'Problem Tracking' sheet - 'Baseline' column: Note the baseline measures for each problem.
Reflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 5.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- The clinical reasoning steps in this section very much relate to one another and help you work toward the final problem list and hypothesis & rationale list. Precise and specific lists will make the rest of the clinical reasoning process flow by!
Case details
The following was found in the examination:
Activities & participation
- BBS: total score 47 / 56 - specific items: sit to stand 4; stand to sit 4; transfers 4; standing 2 min 4; sitting 4; standing feet together 4; standing eyes closed 4; functional reach 3 (20 cm); look over shoulder 3 (weight not fully shifted to R); slipper reach (able to pick up the slipper, but needs supervision); 360 degree turn 2 (R 10.8 sec, L 9.7 sec); stool touch 4; tandem stand 2 (able to take a small step independently and hold 30 sec); one-foot stand 3 (R 2.0 sec, L 5.7 sec)
- ABC - scale: total score 68.5 - ABC - scale: specific items - confidence in...picking up a slipper from floor 40%; reaching at eye level 40%; standing on your tiptoes and reaching above head 30%; standing on a chair and reaching for something 10%; sweeping the floor 40%
Body functions & structures
- Alignment: equal weight distribution, trunk mid-line, normal base of support
- Self-initiated sway forward, backward, side-to-side: loses balance control when sway in different directions is done in fast pace. Adding a double task (cognitive, motor) notably reduces balance control.
- Nudge test: able to maintain balance, uses ankle strategy in small pertubation and hip strategy in large pertubation. Ankle dorsiflexion symmetrical in pertubation backward.
- Modified CTSIB: firm surface - EO 30 sec; firm surface - EC 30 sec; foam surface - EO 10 sec; foam surface - EC 8 sec
- Isometric force generation - MRC - scale: R knee extension 4/5; R ankle dorsiflexion 4/5; all others 5/5
- Passive ROM - lower extremity: full L + R
- MAS: L + R 0/4
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; BBS = Berg Balance Scale; ABC - scale = Activities-specific Balance Confidence - scale; CTSIB = Clinical test of Sensory Interaction and Balance; MRC - scale = Medical Research Council - scale; ROM = range of motion; MAS = Modified Ashworth Scale; R = right; L = left; DF = dorsiflexion; EO = eyes open; EC = eyes closed.
Rationale & evidence
The hypothesised underlying impairments were refined to specific hypotheses based on the examination findings.
- H1 Impaired motor component of balance strategy is refined to 'H1 Impaired anticipatory component of postural control' based on the findings when testing alignment, self-initiated sway and the Nudge test.
- H2 Impaired sensory component of balance strategy is refined to 'H2 Impaired somatosensory component of balance strategy' based on the findings in the mCTSIB test.
- H4 Decreased LE force generation is refined to 'H4 Decreased force generation of right knee extensors and ankle dorsiflexors' based on the findings in manual muscle testing.
- H5 and H6 are refuted based on the findings in PROM and MAS.
Goals
Actions to take
Specify existing problems
- Review the Case details below.
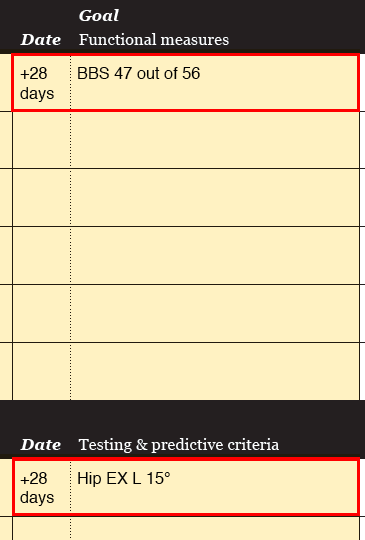
- Establish goals for all problems by setting a target level for the functional measures. Determine when you can expect the patient to meet the goal and set dates of reassessment accordingly.
- Establish testing criteria for each hypothesis. Determine when you can expect the patient to meet the testing criteria and set dates of reassessment accordingly.
Canvas - 'Problem Tracking' sheet - Goal column: Note goals for functional measures and testing criteria. Note dates of reassessment.
Canvas exampleSpecify anticipated problems
- Establish predictive criteria for each anticipated problem. Determine when the predictive criteria should be achieved for the problem to be eliminated. Set dates of reassessment accordingly.
Canvas - 'Problem Tracking' sheet - Goal column: Note goals for functional measures and predicitive criteria. Note dates of reassessment.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 6.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- When you follow the points in the 'Actions-to-take' list, you will automatically have the basis of your SMART- goals on the Canvas. Smart, isn't it!
- Despite of the smart Canvas, writing SMART-goals can be a little tricky sometimes. You could check this practical guide (Bovend'Eerdt et al. 2009) for extra advice. Step 1 is about writing SMART-goals.
Case details
Anna's goals
Anna's expectations for the rehabilitation period: "I want to be confident that I maintain my balance when I do activities that include reaching forward, picking up something from the floor, turning to look behind my shoulder or turning around quickly. Those are activities I continuously need to do in my job".
The final problem list (E= existing, A = anticipated)
P1 Lack of confidence in balance when reaching forward, picking up something from floor, looking over shoulder or turning around. (E)
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; BBS = Berg Balance Scale; ABC - scale = Activities-specific Balance Confidence - scale; CTSIB = Clinical test of Sensory Interaction and Balance; MRC - scale = Medical Research Council - scale; ROM = range of motion; MAS = Modified Ashworth Scale; R = right; L = left; DF = dorsiflexion; EO = eyes open; EC = eyes closed.
Rationale & evidence
When a goal was set to achieve an improvement, the measure was set to reflect minimal detecable changes. Several reference values for minimal detectable changes specific for persons with MS (pwMS) are available (Paltamaa 2008). When they were not available, the general rule of 20% change was applied (Schwid et al. 2002).
Intervention strategy
Actions to take
Plan intervention strategy
- Review the Case details below.
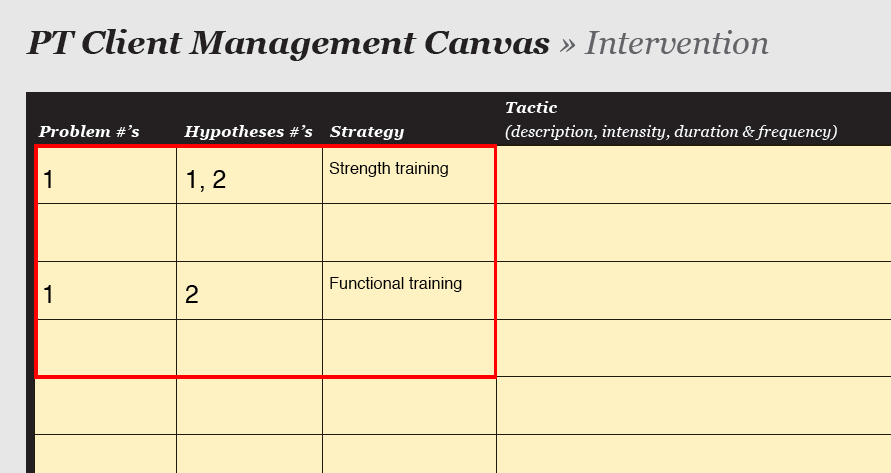
- Plan the intervention strategy. Briefly explain why the strategy should lead to changes in testing & predictive criteria.
- Consider the environmental factors given in the Case details when planning the interventions.
Canvas - 'Intervention' sheet - 'Strategy': Note the strategy and (very) brief reasoning for it.
Canvas examplePlan tactics
- Plan the tactics and relate each tactic to a hypothesis.
- Specify progression.
- Specify the implementer.
Canvas - 'Intervention' sheet - 'Tactics', 'Progression & Remarks', 'Implementer': Note the relevant information.
Canvas exampleReflect, review & continue
- Click on 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as the foundation for the next section.
- Continue to section 7.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- It's good to consider the individual, task and environment in the intervention strategy.
Case details
Goals
- Increased ability to maintain balance: 52 / 56 points on BBS
- Increased confidence in maintaining balance: 82.5 / 100 on ABC-scale
Testing criteria
- Able to maintain balance in self-initiated sway in fast pace
- Able to stand on a foam with EO for 13 sec and EC for 11 sec
- Able to maintain balance in fast pace self-initiated sway & double-task
- Maintain muscle force generation capacity
Environmental factors
- Available individual PT intervention hours : 6 x 45 min in 14 days. Rehabilitation period is in September.
- Inpatient rehabilitation centre with a large very well-equipped exercise hall, well-equipped gym, outdoor recreation area, trampoline.
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; BBS = Berg Balance Scale; ABC - scale = Activities-specific Balance Confidence - scale; CTSIB = Clinical test of Sensory Interaction and Balance; MRC - scale = Medical Research Council - scale; ROM = range of motion; MAS = Modified Ashworth Scale; R = right; L = left; DF = dorsiflexion; EO = eyes open; EC = eyes closed.
Rationale & evidence
Problem - specific activities and tasks that provide a challenge for the multiple systems involved in balance control are used. This approach seems to be more effective than exercises targeting a single system. The activities and tasks are systematically progressed from easy to challenging (Shumway-Cook et al. 2012).
Progressive resistance exercise (PRE) is included as an additional strategy for training of muscle force generating capacity. PRE is well-tolerated by persons with MS (pwMS) and offers a way to improve muscle power. However, when used as a sole intervention strategy it does not seem to improve balance in pwMS (DeBolt et al. 2004, Shumway-Cook et al. 2012).
Reassessment
Actions to take
Review reassessment findings
- Review the progress notes and reassessment findings in the Case details below.
- Report the reassessment findings for the goals and testing & predictive criteria.
Canvas - 'Problem tracking' sheet - 'Progress / discharge' column: note the findings of functional measures and testing & predictive criteria.
Canvas exampleReassess existing problems
- Have the HOAC II - Part 2 algorithm in hand. (If you're still missing it, you can get it here.)
- Follow the 'Reassessment of Existing Problems'.
Reassess anticipated problems
- Have the HOAC II - Part 2 algorithm in hand. (If you're still missing it, you can get it here.)
- Follow the 'Reassessment of Anticipated Problems'.
Reflect, review & continue
- Click 'Show Canvas' in the 'Solution, rationale & evidence' section below.
- Compare your solution with the validated solution.
- Check the rationale for the validated solution and the evidence used.
- Notice that the validated solution is used as a foundation for the next section.
- Continue to the summary.
Download the filled Canvas to catch up to the current step of the case
Filled Canvas- Realise that after this step you have gone through the whole 4-page HOAC II algorithm. It wasn't that indimitating after all, was it?
Case details
Reassessment findings
- BBS 52 / 56
- ABC 80 / 100
- Self-initiated sway: able to maintain balance in self-initiated sway in fast pace and when double-task is added.
- mCSTIB: foam - EO 20.3 sec; foam - EC 11.9 sec
- Isometric MRC: R knee extension 4/5; ankle dorsiflexion 4/5
Solution, rationale & evidence
Solution
Abbreviations used in the Canvas: E = existing (problem); LE = lower extremity; BBS = Berg Balance Scale; ABC - scale = Activities-specific Balance Confidence - scale; CTSIB = Clinical test of Sensory Interaction and Balance; MRC - scale = Medical Research Council - scale; ROM = range of motion; MAS = Modified Ashworth Scale; R = right; L = left; DF = dorsiflexion; EO = eyes open; EC = eyes closed.
Reassessment of existing problems
Have the goals been met? BBS - yes; ABC - scale - no.
- BBS: Measurements indicate that testing criteria have been met. Based on the measurements, the credibility of the hypotheses can be accepted.
- ABC - scale:
- Do measurements indicate if the testing criteria have been met? yes
- Is each hypothesis appropriate and are the testing criteria correct for that hypothesis? yes
- No testing criteria was considered needing revision.
Rationale & evidence
Two weeks is a very short time to note changes at participation level. The ABC -scale measures confidence in different activities. As noted earlier, we must be careful with the interpretation of the results of the ABC - scale as Anna has not performed the activities asked in the questionnaire in her work environment. The result in the scale, however, gives us an indication about Anna's increased confidence in her balance.
Summary
- Well done! Now what? maybe get a cup of tea, rest, digest... and be sure to come back for more later!
Now you have got the hang of the basics of the HOAC II way of clinical reasoning. Very nice! You may want to check out the complete HOAC II algorithm (part 1 and part 2) and grasp the full picture of the process you have gone through. You might feel the need to brush up your knowledge of the HOAC II - the article by Rothstein et al. (2003) has a lot of nice information. Otherwise, you could just continue developing your clinical reasoning skills with a medium level case here on getptsmart.com and build up your knowledge of the HOAC II as you go.
Disclaimer
The foundation of this case study is based on a real patient case. However, the name and personal details have been changed and some case details modified. Any full resemblance to a real person is purely coincidental.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}